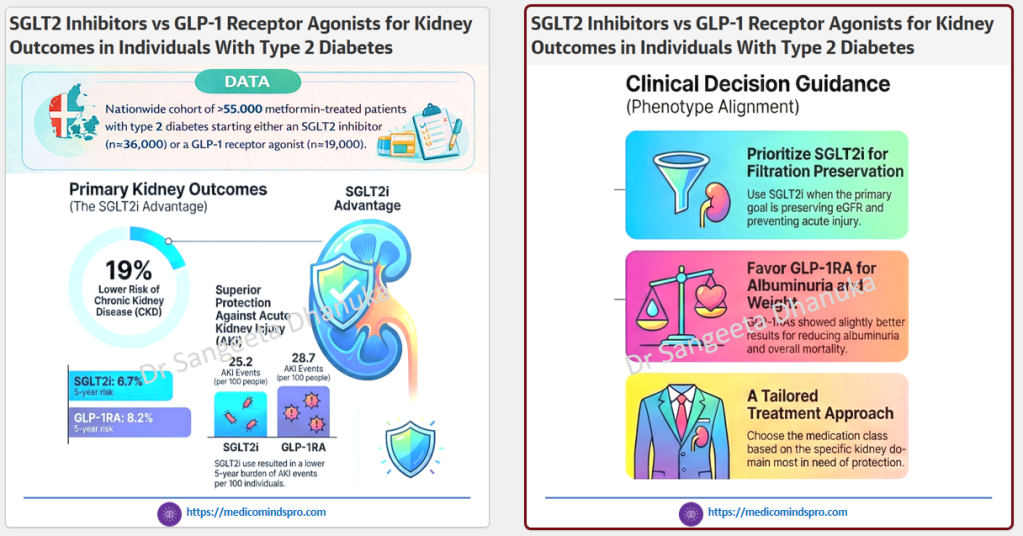
22 Feb 2026: SGLT2i vs. GLP-1RA: Which Protects the Kidneys Better in patients with diabetes?
🟣 >55,000 metformin-treated patients
🟣 Follow-up: Up to 5 years (through 2024)
Initiating an SGLT2 inhibitor was associated with better kidney protection compared with GLP-1 receptor agonists, particularly for the prevention of CKD and acute kidney injury in type 2 diabetes.
For clinicians and healthcare decision-makers:
🟣 Consider the kidney risk profile when choosing the next therapy after metformin.
🟣 Prioritize SGLT2 inhibitors in patients where CKD prevention is a primary goal.
🟣 Use GLP-1 receptor agonists strategically for complementary benefits (weight, albuminuria, cardiometabolic risk).
🟣 Move toward combination and individualized treatment pathways
You can access the study here https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2843983
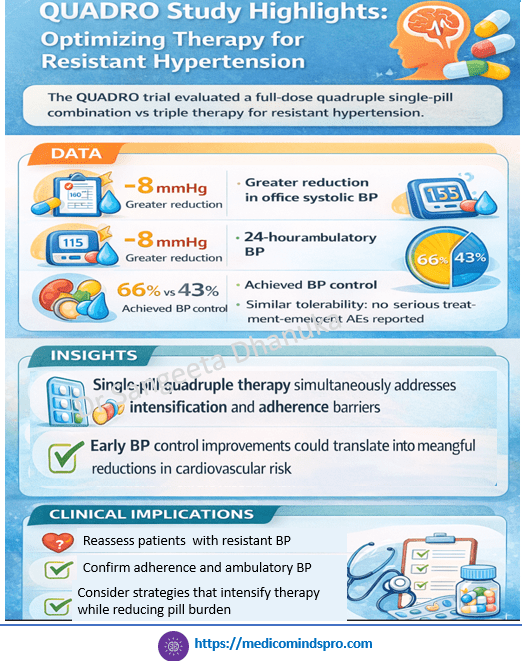
13 Feb 2026: Quadruple vs triple therapy for resistant hypertension: the QUADRO trial
🩺 Quadruple fixed-drug combination effective in resistant hypertension
True resistant hypertension often reflects multiple pathophysiological drivers requiring multi-mechanistic therapy. Many patients remain uncontrolled on triple therapy, and guidelines suggest 4 therapies
1. ACEi/ARB
2. Ca channel blocker
3. Diuretic
4. beta blocker
However, when pill burden rises, adherence falls. The QUADRO study shows that the use of a quadruple FDC (4 different drug classes in accordance with guidelines) in daily clinical practice may prove more effective in controlling BP than other therapeutic options that add further pills to the patient’s treatment regimen. https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehag022/8471744?login=false
9 Feb 2026: Case Report: Euglycemic ketoacidosis in a non-diabetic patient: a rare adverse effect of SGLT2 inhibitor therapy
A recent case report describes a 58-year-old non-diabetic Indian patient with heart failure who developed severe euglycemic ketoacidosis shortly after initiation of SGLT2i for hashtag#heartfailure
The case shows how the absence of hyperglycemia can mislead the diagnosis, especially when presenting symptoms are nonspecific (nausea, vomiting, fatigue).
✅ Clinical takeaway:
In patients on SGLT2 inhibitors, normal glucose does not exclude ketoacidosis. Ketone testing should be considered in unexplained metabolic acidosis or persistent GI symptoms.
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2025.1746210/full
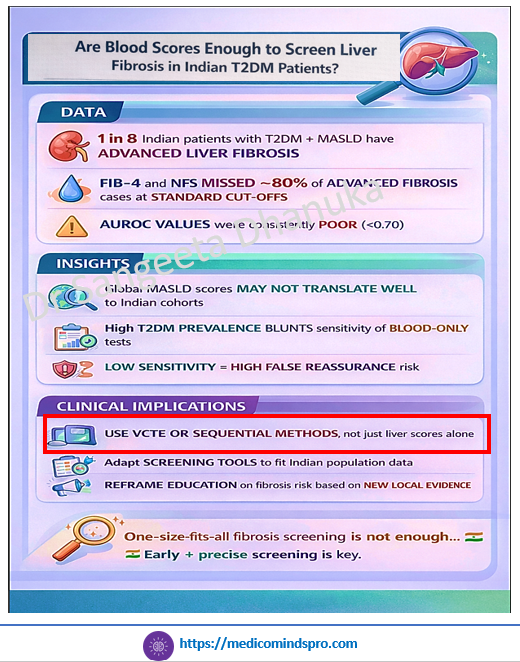
5 Feb 2026: Performance of fibrosis-4 and NAFLD fibrosis score for screening liver fibrosis in Indian individuals with type 2 diabetes
This Indian study used Blood-based non-invasive tests Fibrosis-4 (FIB-4) and NAFLD fibrosis score (NFS), to detect MASLD in Indian patients with diabetes. The results were compared with vibration-controlled transient elastography (VCTE) to assess liver stiffness measurement, which is a good marker of fibrosis.
It was found that the performance of FIB-4 and NFS to predict or rule out advanced fibrosis was poor in Indian patients with type 2 diabetes mellitus and MASLD. In Indian patients with T2DM, these scores missed ~80% of advanced fibrosis
The data indicate that global cutoffs for non-invasive tests may not be relevant for Indian patients, and many patients with MASLD might miss the diagnosis. https://www.sciencedirect.com/science/article/abs/pii/S187140212600007X?via%3Dihub
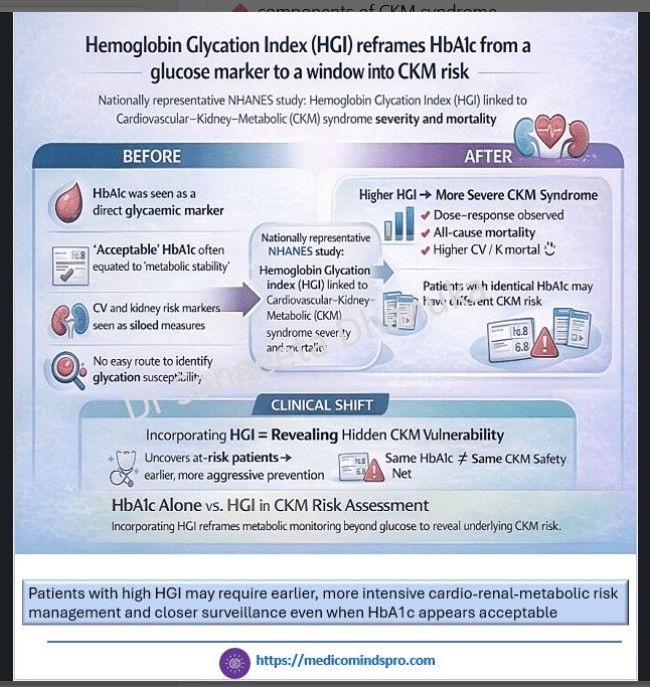
1 Feb 2026: Association of hemoglobin glycation index with the severity and mortality of cardiovascular-kidney-metabolic syndrome
🟣 Glycated hemoglobin (HbA1c) serves as an indicator of average blood glucose levels over the past 2–3 months but it cannot predict the risk of CRM
🟣 Hemoglobin Glycation Index (HGI) reflects individual variation between measured HbA1c and predicted HbA1c from plasma glucose
🟣 This study explored whether HGI is associated with CKM syndrome severity and mortality in 14,680 adults
🟣 It was found that higher HGI was independently associated with more severe CKM syndrome and mortality risk, independent of HbA1c level
🟣 Patients with high HGI may require earlier, more intensive cardio-renal-metabolic risk management and closer surveillance even when HbA1c appears acceptable
https://link.springer.com/article/10.1186/s40842-025-00262-4
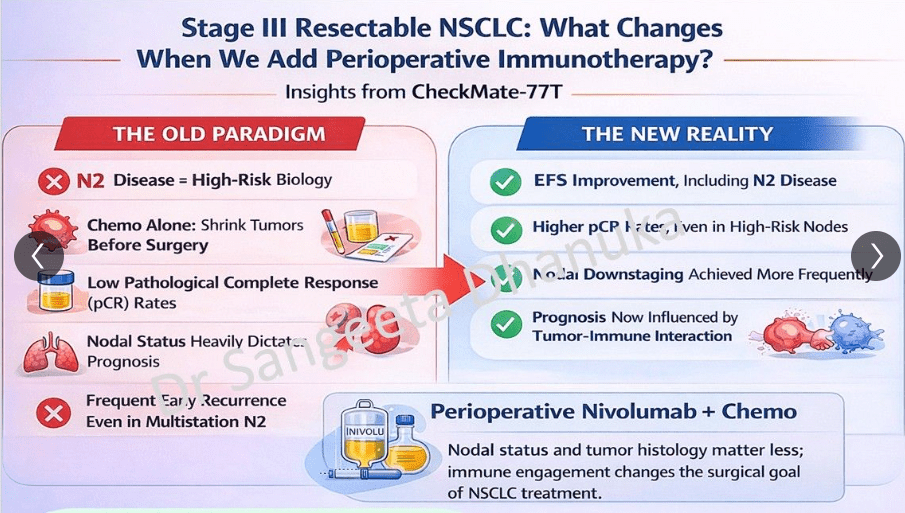
28 Jan 2026: Clinical outcomes with perioperative nivolumab by nodal status in patients with stage III resectable NSCLC: phase 3 CheckMate 77T exploratory analysis
Data to clinical INSIGHTS and implications: The ONE BIG message from CheckMate 77T exploratory analysis
🫁 N2 nodal status in NSCLC may no longer necessarily predict poor outcomes in the era of immunotherapy-based perioperative regimens
🫁 This exploratory analysis of the CheckMate 77T trial evaluated the efficacy and safety of perioperative nivolumab (neoadjuvant nivolumab plus chemotherapy followed by surgery and adjuvant nivolumab) vs a placebo regimen in patients with resectable stage III non-small-cell lung cancer (NSCLC)
🫁 Historically, N2 status was often viewed as a barrier to successful surgery or a predictor of poor prognosis; however, this study suggests that with perioperative chemoimmunotherapy, N2 status does not necessarily dictate a worse outcome and should not be the sole reason to exclude patients from a surgical approach
🫁 This study shows that using perioperative nivolumab allows the surgeons to perform a more precise and less extensive lobectomy while ensuring improved EFS in these high-risk patients with N2 disease. https://www.nature.com/articles/s43018-025-01104-z
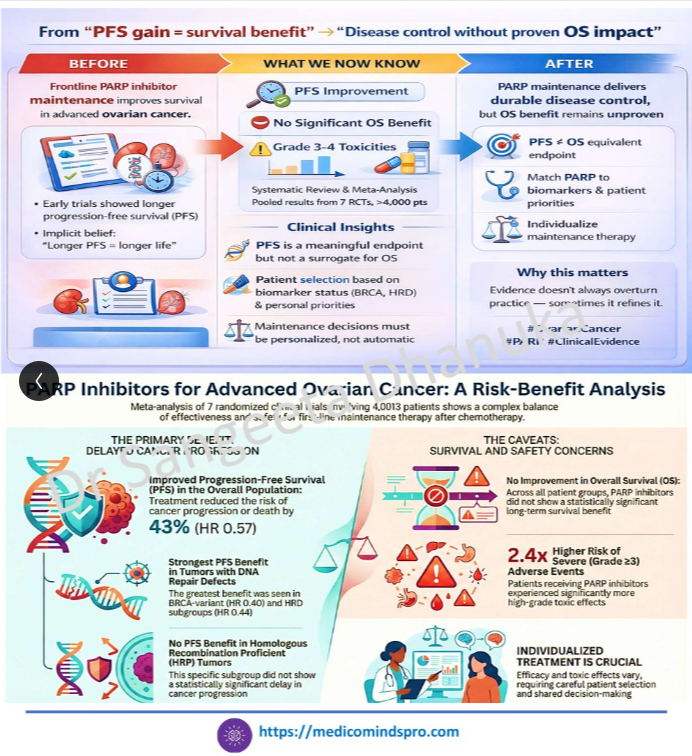
24 Jan 2026: PARP Inhibitor Maintenance After First-Line Chemotherapy in Advanced-Stage Epithelial Ovarian Cancer
PARP inhibitor maintenance after first-line chemotherapy is associated with a clear PFS benefit, but the impact on overall survival remains uncertain. Toxicity profiles and drug-specific differences call for individualized treatment decisions. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2840998
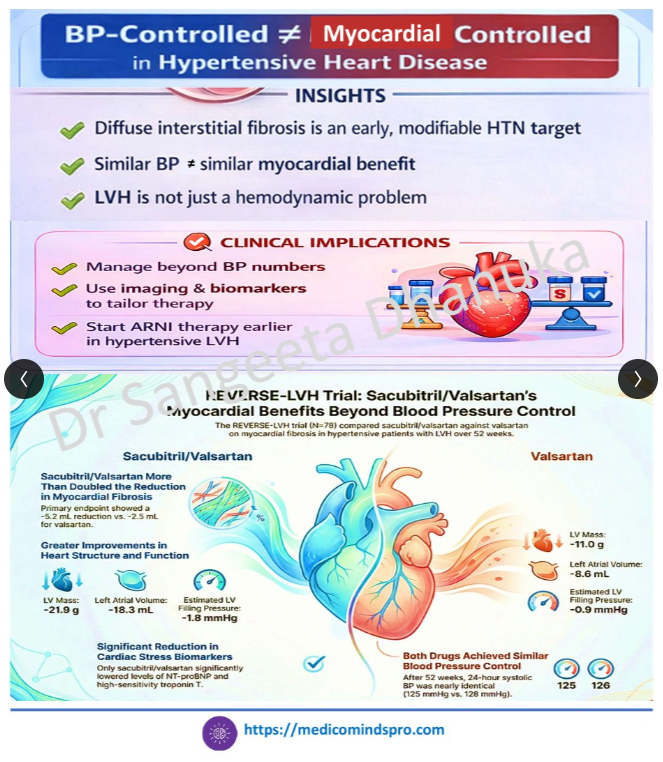
21 Jan 2026: Effects of Sacubitril/valsartan on Hypertensive Heart Disease: the REVERSE-LVH Randomized Phase 2 Trial
Sacubitril/valsartan appears to exert direct anti-fibrotic and reverse-remodeling effects in hypertensive heart disease ( assessed using cardiovascular magnetic resonance) beyond peripheral blood pressure lowering. The findings support targeting myocardial biology—not just BP numbers—early in the hypertensive disease, although larger outcome-powered trials are required https://www.medrxiv.org/content/10.1101/2025.04.08.25325450v2.full.pdf
17 Jan 2026: High-Dose vs Standard-Dose Influenza Vaccine in Older Adults With Diabetes
A recent analysis from the DANFLU-2 randomized clinical trial in JAMA Internal Medicine compared high-dose vs standard-dose influenza vaccines in adults aged 65+ (n > 330,000), including nearly 44,000 people with diabetes. High-dose vaccine recipients experienced lower hospitalizations for cardiorespiratory disease, cardiovascular events, and influenza — and the benefit was consistent irrespective of diabetes status.
These findings reinforce that in older adults — even those with chronic conditions like diabetes — a higher-antigen influenza vaccine may provide stronger clinical protection than standard dosing. Link to the full text https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2843860

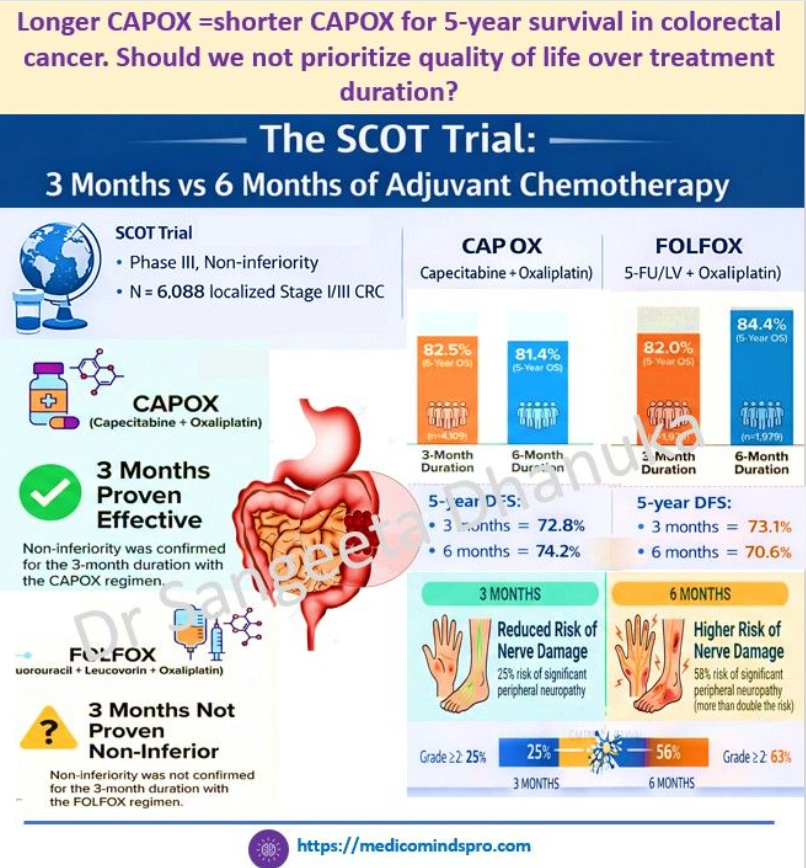
13 Jan 2026: Three Versus 6 Months of Adjuvant Oxaliplatin-Fluoropyrimidine Chemotherapy for Colorectal Cancer: Final Results of SCOT
🟣 In the SCOT trial (n=6,088), 5-year overall survival was identical (82.4%) with 3 vs 6 months of adjuvant oxaliplatin-based chemotherapy.
🟣 CAPOX for 3 months was non-inferior to 6 months for OS.
🟣 Extending treatment to 6 months increased grade ≥2 neuropathy from ~25% to ~58%.
In an era focused on value-based care, duration matters as much as drug choice, especially when long-term toxicity can permanently affect quality of life
When 3 months of CAPOX delivers the same 5-year survival as 6 months—but with half the neuropathy burden, the clinical question shifts from ‘Is it effective?’ to ‘Why are we still overtreating?
Here is the link to the full text: https://ascopubs.org/doi/10.1200/JCO-25-00621
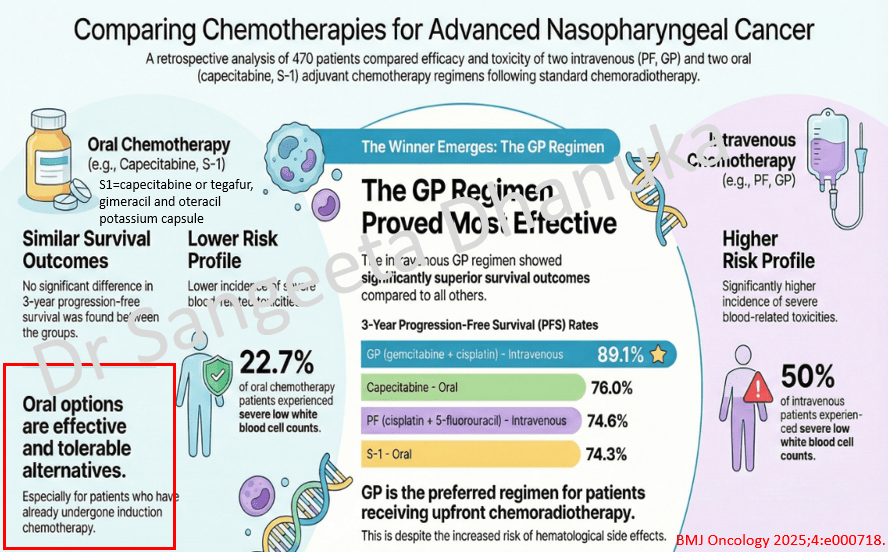
10 Jan 2026: Comparing Adjuvant Chemotherapies for Advanced Nasopharyngeal Cancer
This retrospective study evaluated the efficacy and safety of different adjuvant chemotherapy regimens for patients with locoregionally advanced nasopharyngeal carcinoma following concurrent chemoradiotherapy. The study found no significant difference in progression-free survival (PFS) between intravenous and oral administration. However, within the overall cohort, the GP regimen demonstrated a significantly superior 3-year PFS rate. For patients treated with induction chemotherapy and CCRT, oral chemotherapy, either with capecitabine or S1, was efficacious and tolerable.
The link to the full text is here https://bmjoncology.bmj.com/content/4/1/e000718
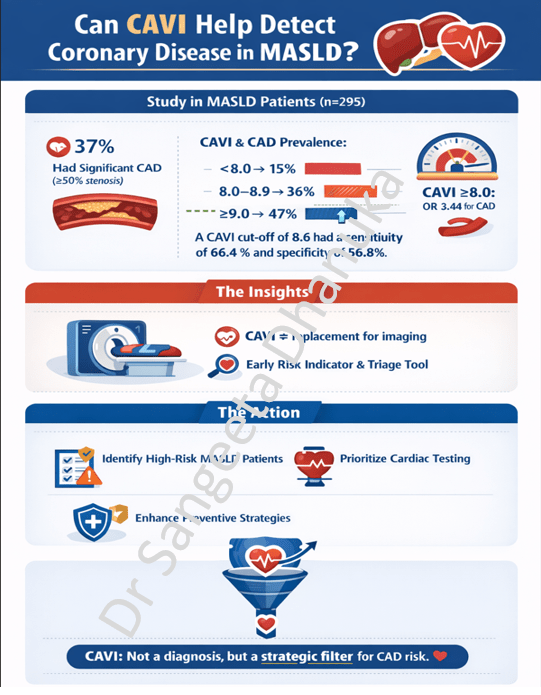
6 Jan 2026: Can CAVI Help Detect Coronary Disease in MASLD?
Patients with metabolic dysfunction–associated steatotic liver disease (MASLD) have a high cardiovascular risk, yet there is no established, practical screening approach for detecting subclinical coronary artery disease (CAD) in this population. Coronary CT angiography (CCTA) is effective but resource-intensive. The study explores whether CAVI, a non-invasive measure of arterial stiffness, can help fill this gap.
Here is the link to the study. https://doi.org/10.1016/j.jjcc.2025.12.006
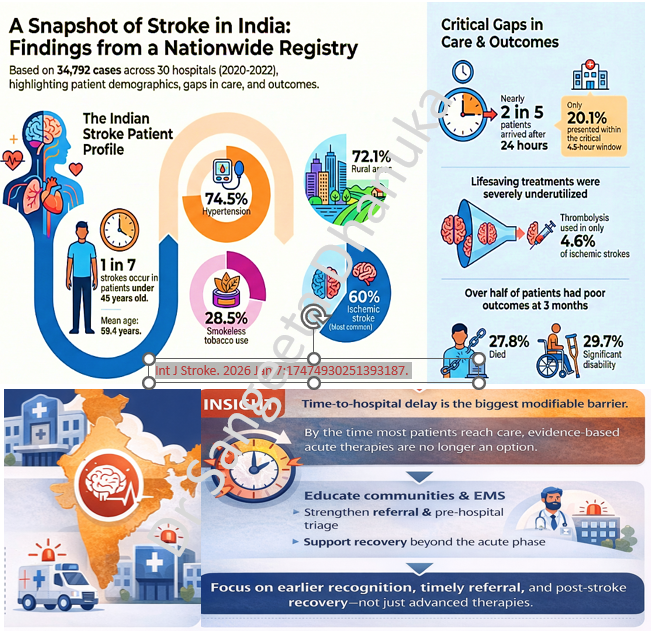
2 Jan 2026: A Snapshot of Stroke in India: Findings from a Nationwide Registry
This prospective study, based on the Hospital-Based Stroke Registries analyzed 34,792 stroke cases across 30 centers in India between 2020 and 2022 to identify patterns, risk factors, and long-term outcomes. The study highlights that stroke in India affects a relatively young population, and the rural incidence being very high. The data reveals a significant public health challenge characterized by late hospital arrival and underutilized acute treatments.
Here is the link to the study https://journals.sagepub.com/doi/10.1177/17474930251393187
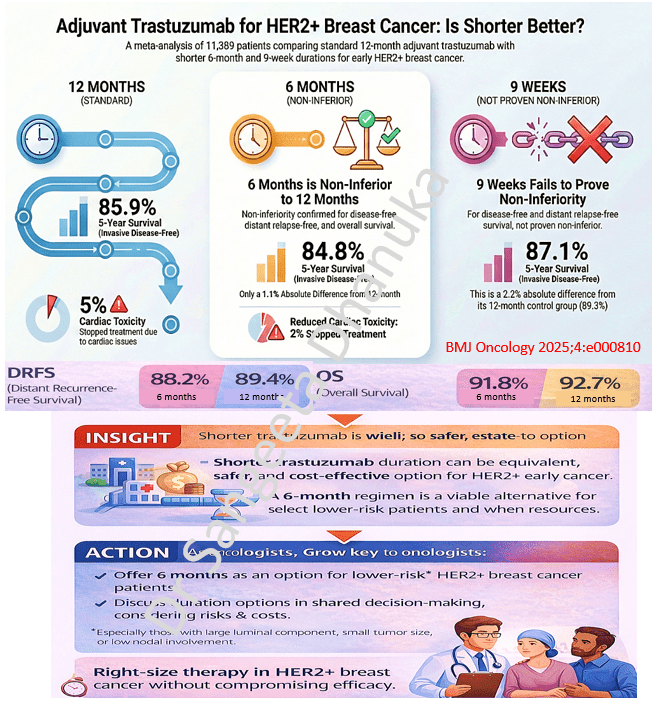
29 Dec 2025: Adjuvant Trastuzumab for HER2+ Breast Cancer: Is Shorter Better?
This systematic review and meta-analysis of 5 phase III non-inferiority trials, involving 11,389 patients, evaluated whether shorter durations of adjuvant trastuzumab are as effective as the standard 12-month regimen for HER2-positive early breast cancer. The study is unique as it is the first to utilize individual patient data (IPD) for this comparison, providing more reliable results than previous analyses. Based on this meta-analysis, 6 months of trastuzumab is a safe and effective option, specifically for patients at low risk of recurrence—those with small, node-negative, and ER-positive tumors. The study suggests that adopting a 6-month schedule can help patients avoid unnecessary physical, psychological, and financial toxicities while retaining nearly all the survival benefits of the longer course.
Here is the link to the full text https://bmjoncology.bmj.com/content/bmjonc/4/1/e000810.full.pdf
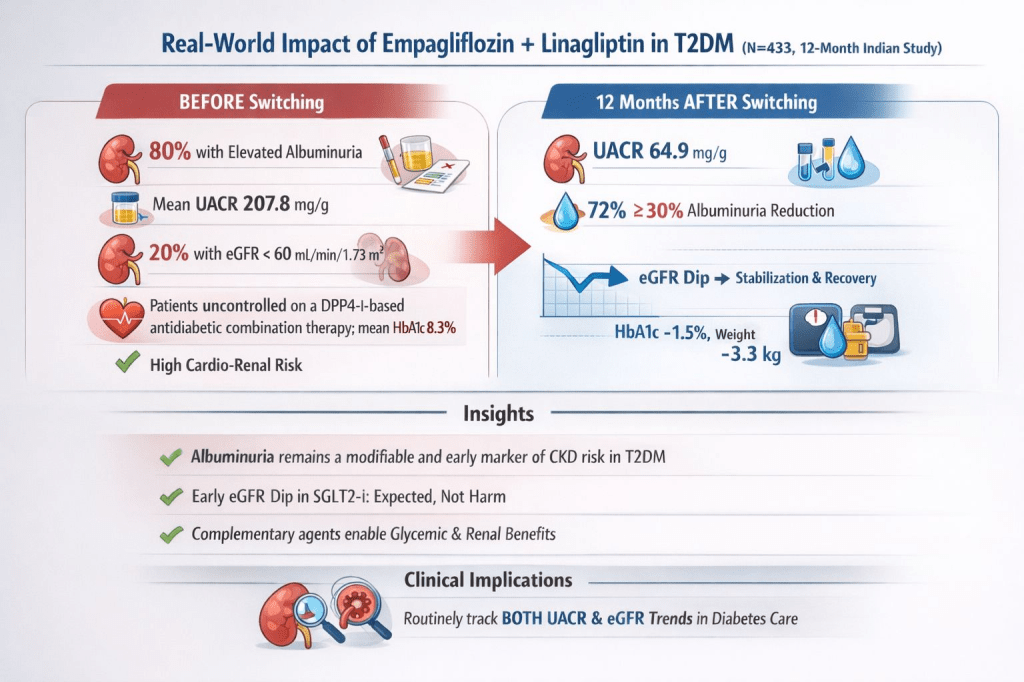
26 Dec 2025: Effectiveness of Empagliflozin-Linagliptin Fixed-Dose Combination on Chronic Kidney Disease Outcomes in Patients With Type 2 Diabetes in a Real-World Setting
A recent 12-month Indian real-world study in adults with type 2 diabetes evaluated renal outcomes after initiating a fixed-dose combination of empagliflozin + linagliptin in SGLT2i–naïve patients previously uncontrolled on DPP-4 inhibitors. In this observational study, the use of FDC of empagliflozin and linagliptin for at least 12 months in T2DM patients previously uncontrolled on a DPP4-i-based regimen was associated with reductions in albuminuria and improvement in eGFR slope after the expected initial dip at three months. Improvements in glycemic control and body weight were also observed, regardless of underlying cardiometabolic risk.
The full text of the study is here: https://www.cureus.com/articles/423115-effectiveness-of-empagliflozin-linagliptin-fixed-dose-combination-on-chronic-kidney-disease-outcomes-in-patients-with-type-2-diabetes-in-a-real-world-setting#!/
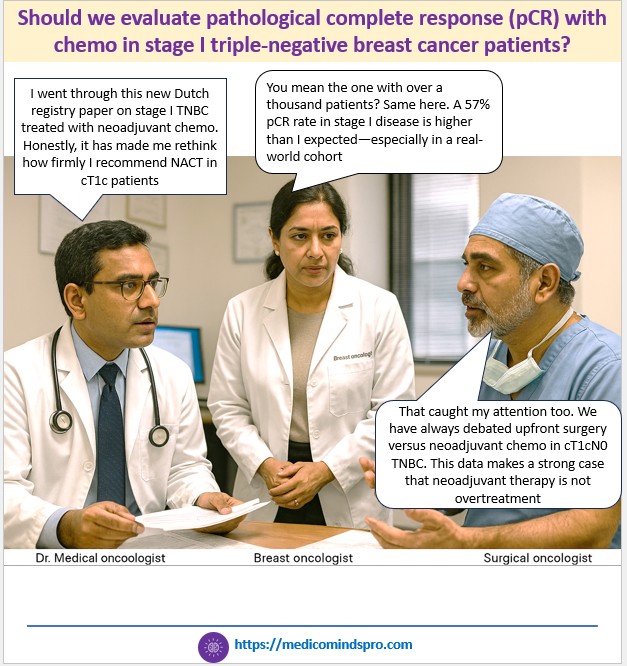
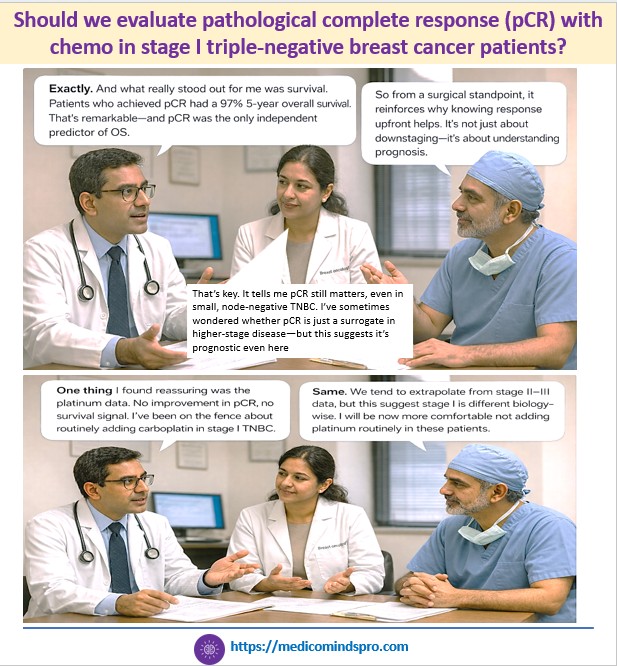
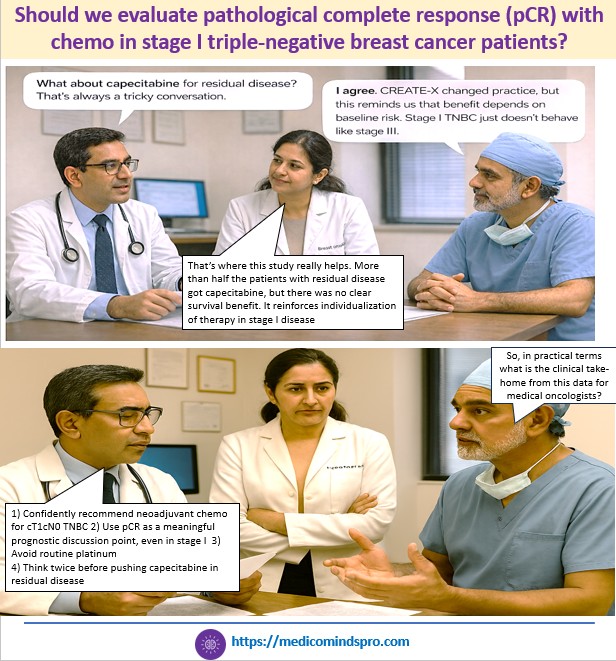
22 Dec 2025: Should we evaluate pathological complete response (pCR) with chemo in stage I triple-negative breast cancer patients?
New study shows prognostic importance of pathological complete response (pCR) to neoadjuvant chemotherapy (NACT) in early-stage triple-negative breast cancer (TNBC)
Importance of the study: Since most clinical trials for TNBC focus on stage II/III, little is known on the impact of NACT in stage I disease
🟣 Patients were treated with anthracycline-taxane-based neoadjuvant chemo, and 57.3% had a pCR
🟣 Platinum-based treatment did not significantly improve the pCR rate
🟣 Patients with residual disease, who received adjuvant capecitabine, did not show significant improvement in OS
🟣 pCR was associated with a favorable long-term outcome
The infographic below shows how this new data might influence conversations between oncologists, and the key implications for clinical practice
The full text of the study is here https://www.esmoopen.com/article/S2059-7029(25)01793-4/fulltext
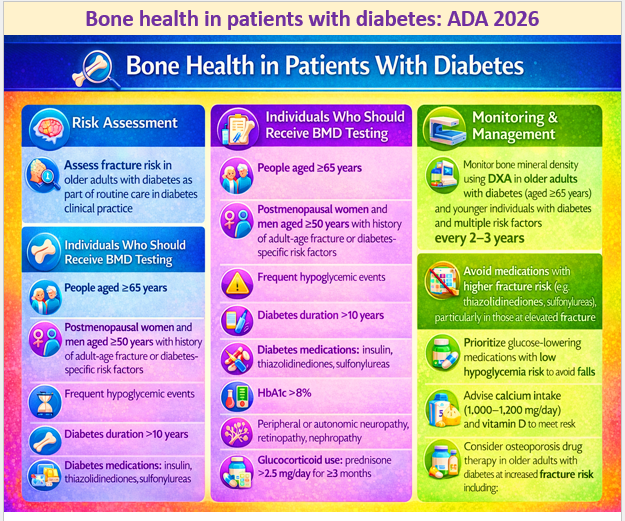
15 Dec 2025: Bone health in patients with diabetes: ADA 2026
Age-specific fracture risk is significantly increased in people with type 1 or type 2 diabetes in both sexes, with a 34% increase in fracture risk compared with those without diabetes
Longer diabetes duration further increases fracture risk
Hence, HCPs should assess fracture history and risk factors in people with diabetes and recommend measurement of BMD if appropriate, according to the individual’s age and sex.
The document provides a detailed discussion, with relevant references on bone health in diabetes and why and how long-term diabetes increases the risk of fracture. The link to the publication is here https://diabetesjournals.org/care/article/49/Supplement_1/S61/163931/4-Comprehensive-Medical-Evaluation-and-Assessment
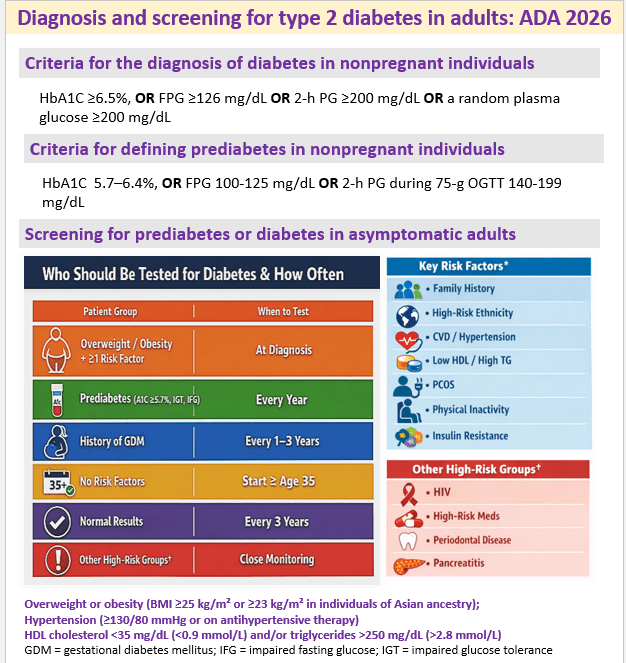
12 Dec 2025: Diagnosis and screening for type 2 diabetes in adults: ADA 2026
The full text on Diagnosis and screening is here https://diabetesjournals.org/care/article/49/Supplement_1/S27/163926/2-Diagnosis-and-Classification-of-Diabetes
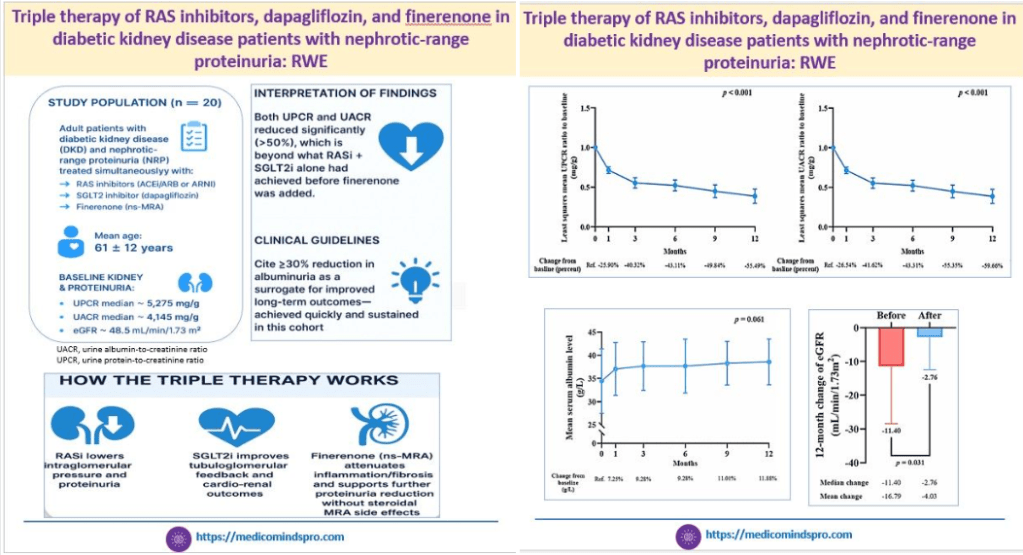
9 Dec 2025: RAS inhibitors+ dapagliflozin + finerenone in diabetic kidney disease with nephrotic-range proteinuria: RWE
This is the first real-world study that evaluated the effects of triple therapy with RAS inhibitors, SGLT2 inhibitors, and finerenone in DKD patients having nephrotic-range proteinuria
The results showed that this triple therapy may be an effective option to reduce proteinuria and albuminuria in such patients, while also slowing chronic kidney disease progression.
The current drawback of the study is the small sample size. But I am sure these outcomes will spur further studies of this triple combination
Here is the link to the study https://www.nature.com/articles/s41598-025-27239-8
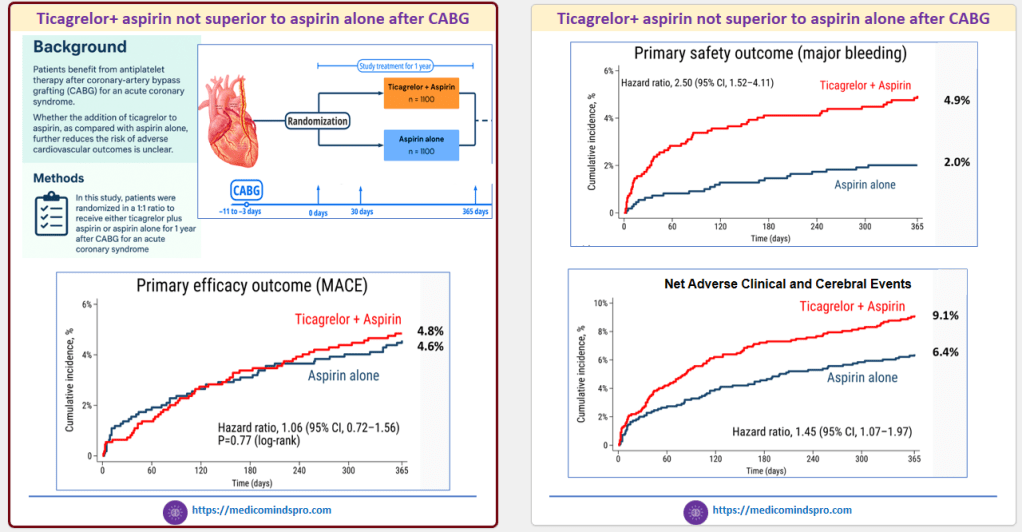
6 Dec 2025: Are we moving to Single antiplatelet therapy (SAPT) even after CABG?
Patients who undergo Coronary-artery bypass grafting (CABG) for an acute coronary syndrome are considered a high-risk group, for whom standard Dual Antiplatelet Therapy (DAPT) is recommended
But the recently published data of the TACSI study show that DAPT for 1 year was not superior to aspirin alone after CABG.
Here is the link to the study https://www.nejm.org/do/10.1056/NEJMdo008283/full/
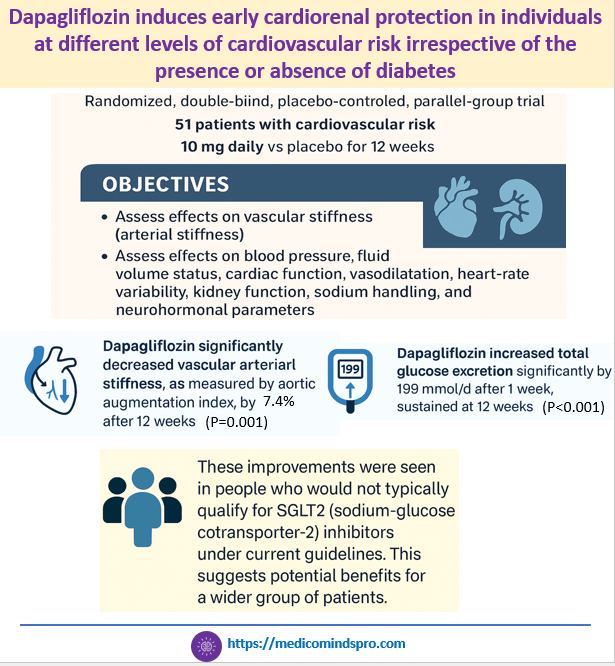
3 Dec 2025: Dapagliflozin induces early cardiorenal protection in individuals at different levels of cardiovascular risk irrespective of the presence or absence of diabetes
This new study slated published in the 2026 issue of Hypertension journal, investigated the cardiorenal effects of dapagliflozin in patients at cardiovascular risk, with or without type 2 diabetes.
It shows that dapagliflozin improves early cardiovascular and kidney health markers after 12 weeks in patients at varying cardiovascular risk, with or without type 2 diabetes. The results show that early use of SGLT2 inhibitors may help prevent cardiovascular and kidney disease in at-risk individuals.
The paper also explains how SGLT2 inhibition leads to cardiovascular and kidney protection. The sample size is small, but it raises the possibility that SGLT2 inhibitors could be effective in the primary prevention of cardiovascular and kidney complications
Here is the link to the full text https://www.ahajournals.org/doi/abs/10.1161/HYPERTENSIONAHA.125.25955?casa_token=Hi2vgrJLxfsAAAAA%3AzNicAQ3JwIoQlcZT2tHaXEgLuDFpWpR6Jq-IsguTx-0FKch8j_pk0MGxNk7N2e6NaMwsWk5PLMLZbQ
30 Nov 2025: MRI-confirmed improvement in MASLD with empagliflozin
While the beneficial effect of SGLT2 inhibitors on MASLD in patients with diabetes is known, most studies have used only fibrosis indices or liver ultrasound for evaluation
This study used MRI for evaluation. Most patients had grade 2 or 3 steatosis on MRI at baseline. There was a confirmed greater improvement in the empagliflozin group, with 94% showing grade 1 or lower steatosis on ultrasound and 100% achieving grade 0 on MRI (p < 0.001 for both).
Here is the link to the study https://pmc.ncbi.nlm.nih.gov/articles/PMC12664258/
The graphic below is a depiction of how the study might shape conversations between HCPs and patients
22 Nov 2025: New hope for patients with oral steroid-dependent, severe, uncontrolled asthma
The WAYFINDER study evaluated the ability of tezepelumab to enable patients with oral steroid-dependent, severe, uncontrolled asthma to reduce or discontinue oral steroid (OCS) use without loss of asthma control.
After 52 weeks, nearly 90% of patients had a maintenance OCS dose of 5 mg/day or less, and more than 50% completely discontinued OCS. The graphics below convey the patient benefits through emotions involving not just the patient but the caregiver and clinician, too.
Read the full text here: https://www.thelancet.com/journals/lanres/article/PIIS2213-2600(25)00359-5/fulltext

19 Nov 2025: Triple Versus Dual Lipid-Lowering Therapy in Acute Coronary Syndrome
This study compared the efficacy and safety of triple LLT (high-dose, high-intensity statin+ezetimibe+bempedoic acid) vs standard of care (high-dose, high-intensity statin+ezetimibe) after ACS
Adding bempedoic acid to statin–ezetimibe therapy in the setting of ACS was safe but failed to improve the percentage of patients achieving the LDL-C goal (<55 mg/dL) at 8 weeks.
Here is the link to the publication https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.125.075388
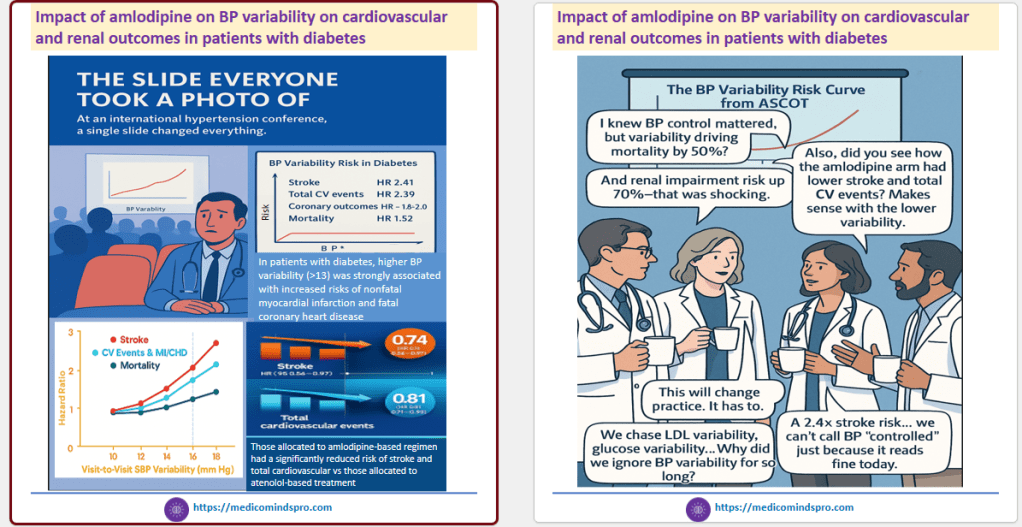
16 Nov 2025: Impact of amlodipine on BP variability on cardiovascular and renal outcomes in patients with diabetes
This study evaluated the relationship between visit-to-visit BPV and cardiovascular events, renal outcomes, and mortality in individuals with and without diabetes, using data from the ASCOT trial
Authors suggest that long-acting calcium channel blockers should be included into treatment strategies to improve cardiovascular outcomes.
The infographics below show how this data can be shared creatively in CME slide decks or through in-clinic communication
Here is the link to the publication https://journals.lww.com/jhypertension/abstract/2025/12000/the_impact_of_blood_pressure_variability_on.15.aspx
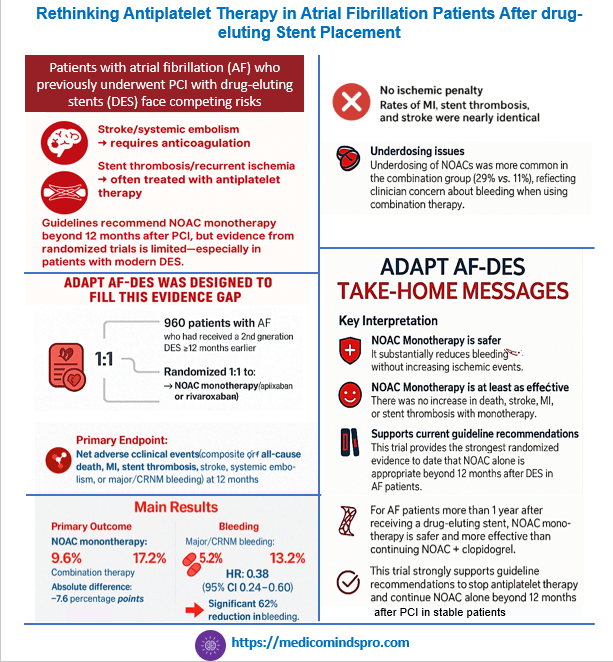
13 Nov 2025: Rethinking Antiplatelet Therapy in Atrial Fibrillation Patients After drug-eluting Stent Placement
A recently published study has shown that among patients with atrial fibrillation who had undergone implantation of a drug-eluting stent at least 1 year earlier, NOAC monotherapy was noninferior to combination therapy for net adverse clinical events.
This data strongly reinforces the ESC and ACC/AHA guidelines to stop antiplatelet therapy and continue NOAC alone beyond 12 months after PCI in stable patients.
This is now the most robust randomized evidence supporting NOAC monotherapy in AF patients with prior PCI. The study can be accessed at https://www.nejm.org/doi/pdf/10.1056/NEJMoa2512091
10 Nov 2025: Prasugel-based DAPT better than ticagrelor-based DAPT in Indian patients with Type 1 or Type 2 diabetes who had undergone drug-eluting stent placement
This data from the TUXEDO-2 trial was presented at AHA 2025. It was conducted at 66 centers in India, and included 1,800 adults. This was an interesting result, as currently, these medications are treated as interchangeable. Read more here https://newsroom.heart.org/news/effectiveness-of-anti-clotting-meds-after-stent-placement-varied-in-people-with-diabetes

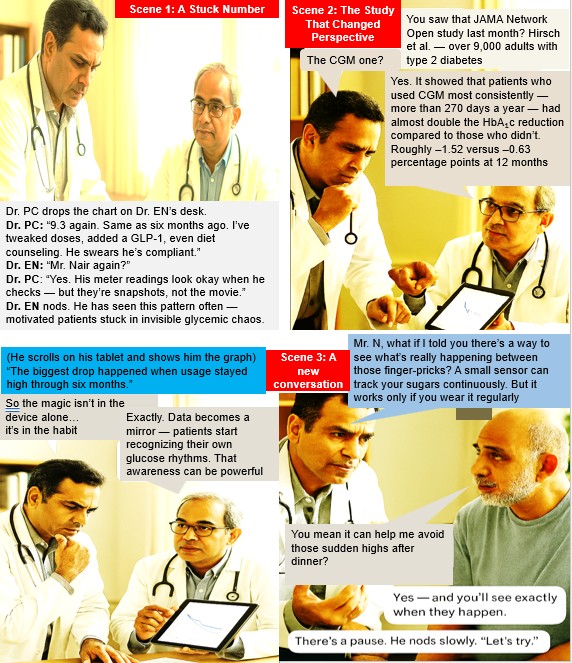
5 Nov 2025: How long should CGM be worn by patients with diabetes for a meaningful difference in glycemic control?
This study in 9258 adults published last week found that wearing CGM for >75% or more of days over the 12-month period was associated with improved glycemic control compared with infrequent or no use of CGM. The study also found that 6 months post-CGM initiation may be a critical time to focus counseling on continuing CGM use, as compliance begins to dip at this time point due to therapeutic inertia. Here is the link to the study https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2840792

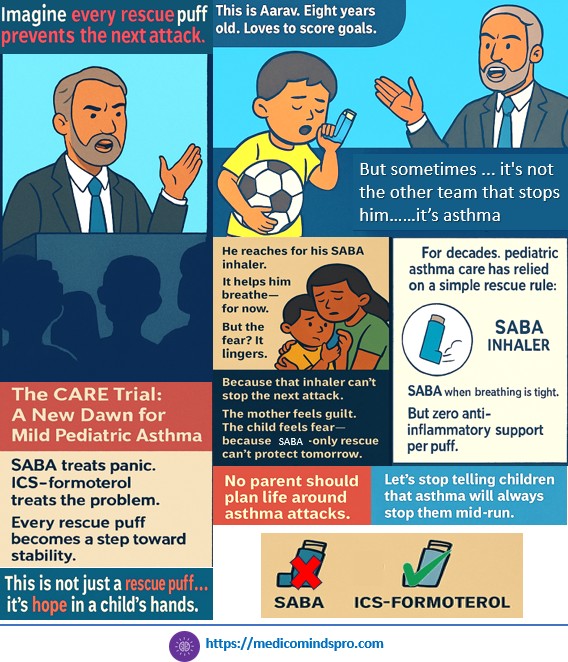
30 Oct 2025: Budesonide–formoterol versus salbutamol as reliever therapy in children with mild asthma (CARE)
The CARE study has shown that Combination inhaled corticosteroid–formoterol reliever monotherapy reduces the rate of asthma attacks compared to short-acting β2-agonist (SABA) reliever monotherapy in children by 45%. The study suggests a New Approach to Acute Pediatric Asthma
Link to the study https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(25)00861-X/abstract
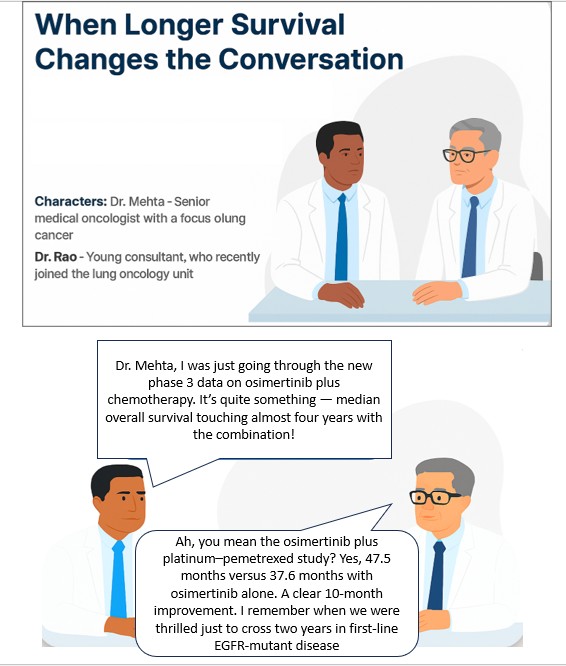
25 Oct 2025: Survival with Osimertinib plus Chemotherapy in EGFR-Mutated Advanced NSCLC
The recently released results of the FLAURA 2 trial are likely to generate considerable interest among oncologists treating lung cancer (NSCLC).
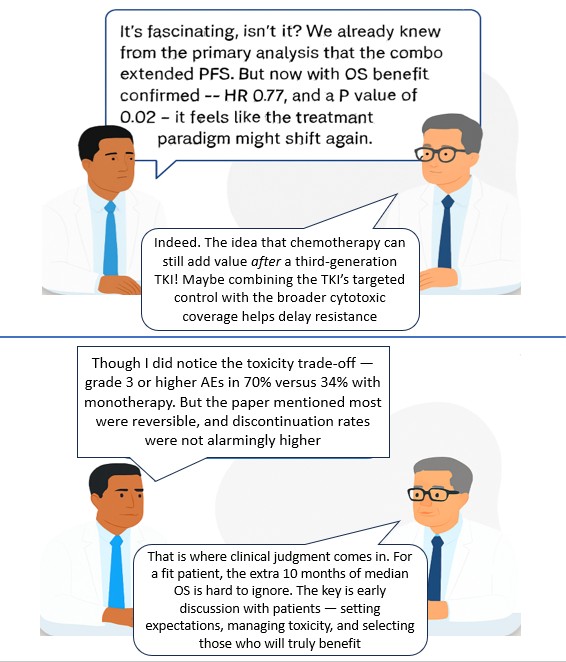
The study showed that in patients with EGFR-mutated (exon 19 deletion or L858R mutation) advanced NSCLC, first-line treatment with osimertinib plus platinum–pemetrexed led to significantly longer overall survival than osimertinib monotherapy. However, it was associated with an increased risk of reversible adverse events of grade 3 or higher.
Right patient selection at the right time will remain the key here. A patient who has perhaps a good ECOG PS and can tolerate the adverse effects better might be the best candidate for this treatment. That will clinically mean it is important to perform NGS testing as soon as possible.
Publication link https://www.nejm.org/doi/10.1056/NEJMoa2510308
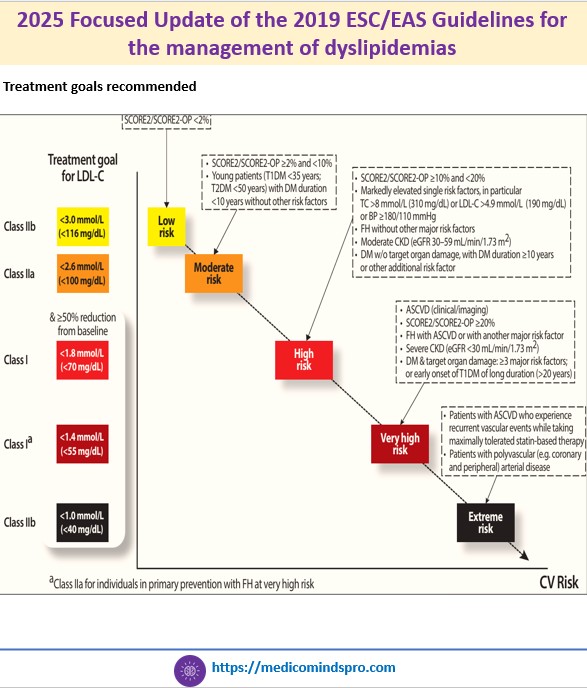
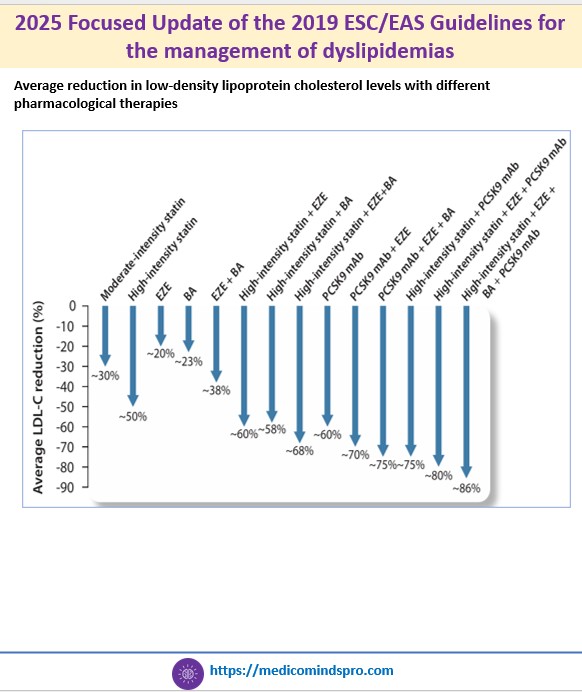
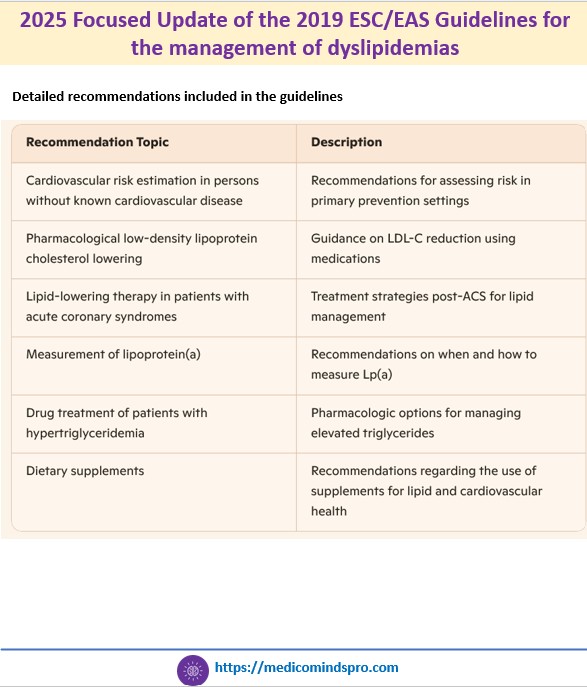
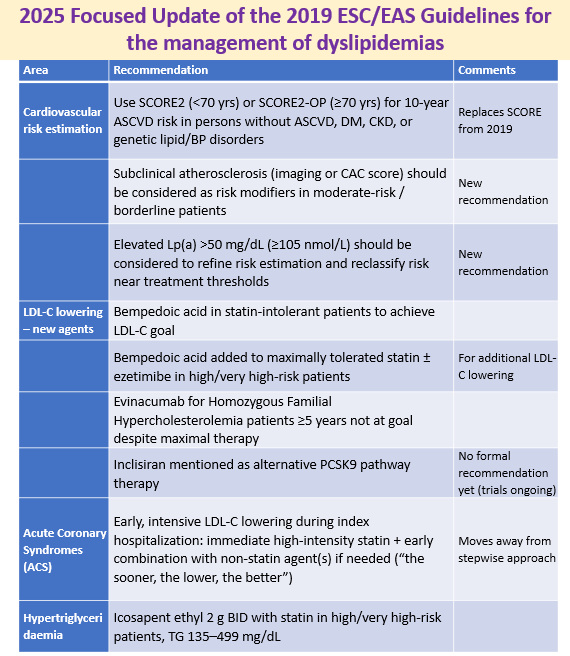
19 Oct 2025: 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidemias
An updated guideline has been published by the ESC and EAS regarding the management of dyslipidemias. All new recommendations included in this Focused Update are an addition to the recommendations of the 2019 ESC/EAS Guidelines and do not replace the 2019 guidelines.
Some highlights include
🟣 The guideline now recommends using SCORE2 and SCORE2-OP, rather than the original SCORE algorithm for risk estimation. These updated tools use non-high-density lipoprotein cholesterol instead of total cholesterol and are calibrated to national CVD mortality rates
🟣 Recommendations on non-statin agents like ezetimibe, PCSK9 inhibitors, or bempedoic acid
🟣 Early and intensive LDL-C lowering during hospitalization for acute coronary syndrome
🟣 The update reinforces that dietary supplements and vitamins lack sufficient evidence
Publication link: https://academic.oup.com/eurheartj/article/46/42/4359/8234482?login=false#529497870


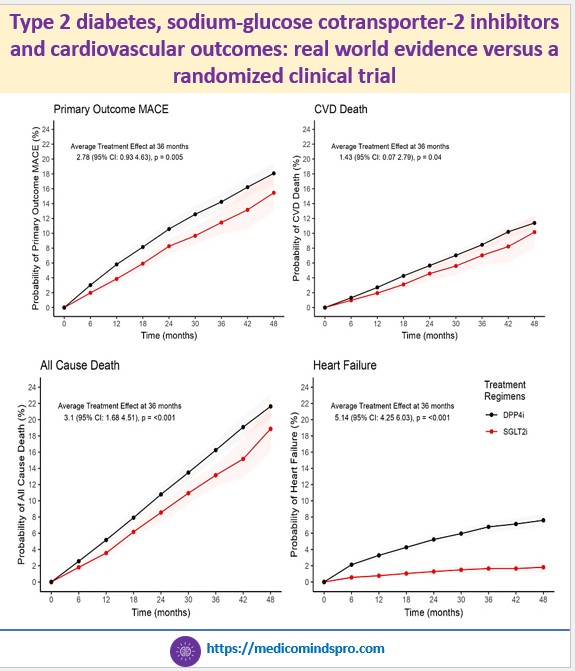
15 Oct 2025: Type 2 diabetes, sodium-glucose cotransporter-2 inhibitors and cardiovascular outcomes: real world evidence versus a randomized clinical trial
A new Danish study published in Cardiovascular Diabetology offered clarity. Using real-world data from over 13,000 patients with T2D and established cardiovascular disease, researchers emulated the EMPA-REG OUTCOME trial—but with a twist: Patients were older, frailer, and less adherent than those in trials. Yet the findings were striking. The benefits were more pronounced in patients over 65 years, showing the therapy’s value where the need is greatest. By mimicking real-world adherence and treatment dynamics, the study reaffirms that SGLT2is provide consistent, clinically meaningful benefits beyond clinical trials.
Publication link: https://cardiab.biomedcentral.com/articles/10.1186/s12933-025-02924-0

9 Oct 2025: Effects of empagliflozin on conventional and exploratory acute and chronic kidney outcomes
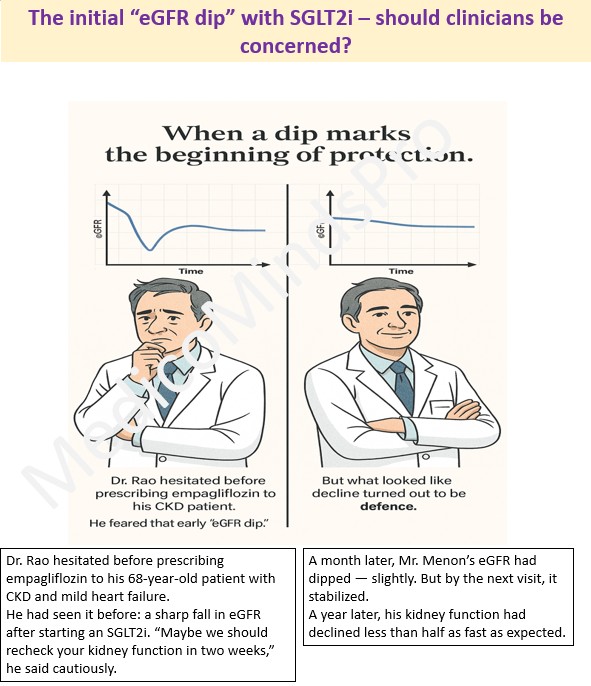
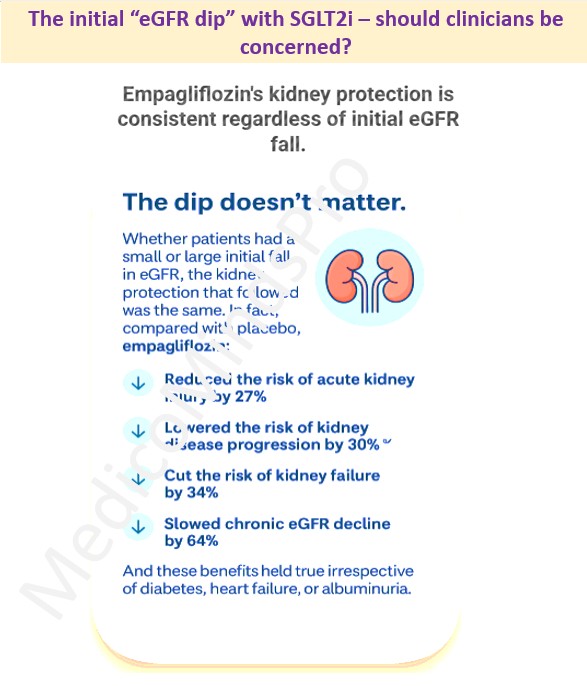
The “eGFR dip” is a psychological barrier for many clinicians — a signal that seems to say ‘wait’. But the latest data from a meta-analysis of over 23,000 participants across four landmark trials — EMPA-REG OUTCOME, EMPEROR-Reduced, EMPEROR-Preserved, and EMPA-KIDNEY — told a different story. Using individual participant-level data, the researchers asked a crucial clinical question: “Does this dip predict harm, or is it simply part of how the drug works?”
The answer: the dip doesn’t matter. Whether patients had a small or large initial fall in eGFR, the kidney protection that followed was the same. The authors suggest that routine early re-testing may be unnecessary because the dip is transient and benign. The conclusion: a transient fall does not equal renal injury — it may signal renal protection taking effect. Read the paper here https://www.thelancet.com/journals/landia/article/PIIS2213-8587(25)00222-0/fulltext

6 Oct 2025: Key changes in the new AHA 2025 hypertension guidelines
The AHA guidelines for hypertension were recently updated. While there is a long list of what is new, there are some updates that most clinicians, including general practitioners, must know. The link to the guidelines is https://www.ahajournals.org/doi/10.1161/CIR.0000000000001356

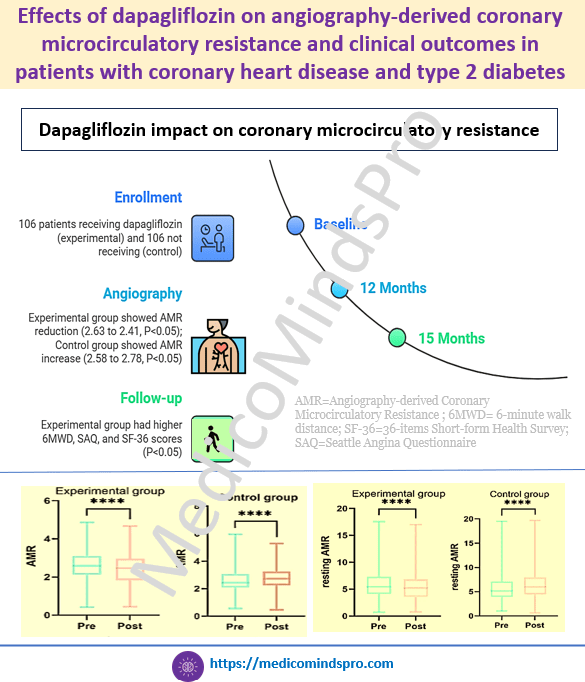
3 Oct 2025: Effects of dapagliflozin on angiography-derived coronary microcirculatory resistance and clinical outcomes in patients with coronary heart disease and type 2 diabetes
Coronary microvascular dysfunction is prevalent in patients with coronary heart disease and Type 2 Diabetes. SGLT2is have cardioprotective effects; however, their impact on microcirculatory function is not known. This study evaluated the effects of dapagliflozin on microcirculatory function and clinical outcomes in patients with CHD and T2DM. Beneficial effects of dapagliflozin were seen on coronary microcirculatory function, exercise capacity, quality of life, and survival in patients with CHD and T2DM.
Here is the study link https://dmsjournal.biomedcentral.com/articles/10.1186/s13098-025-01916-0
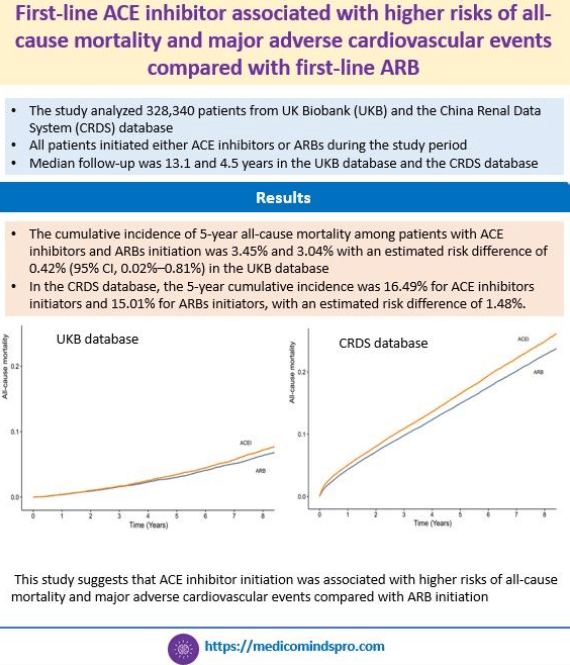
30 Sept 2025: First-line ACE inhibitor associated with higher risks of all-cause mortality and major adverse cardiovascular events compared with first-line ARB
This study shows that shows that ACE inhibitor initiation for hypertension was associated with higher risks of all-cause mortality and major adverse cardiovascular events compared with ARB initiation. This was a comprehensive evaluation based on real-world data from 2 large longitudinal cohorts comparing all-cause mortality between ARBs and ACE inhibitors during a long-term follow-up. This data is important because guidelines for managing hypertension and chronic kidney disease generally do not discriminate between ACE inhibitors and ARBs in recommending one over the other
Here is the full text link: https://www.ahajournals.org/doi/pdf/10.1161/HYPERTENSIONAHA.125.25549
26 Sept 2025: Practical Recommendations on Sunscreen Use for Indians
The way this consensus is written is likely to be useful for common people as well because it also provides details on what the labels on sunscreen packs mean and what to check besides the SPF. The statements are a mix of tables and graphics- I would say a more interesting way to present them. This is the era of media and graphics, and using them creatively in publications certainly enhances the presentation. Check the full text here https://pmc.ncbi.nlm.nih.gov/articles/PMC12439021/#jocd70441-sec-0042

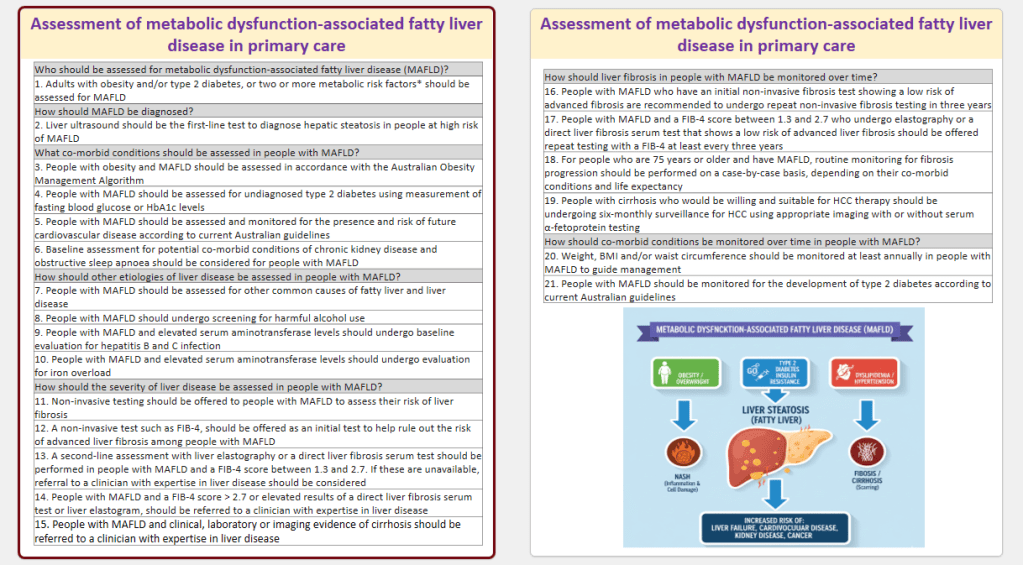
23 Sept 2025: Assessment of metabolic dysfunction‐associated fatty liver disease in primary care
This evidence‐based consensus statement summary provides recommendations for the assessment and monitoring of adults with MAFLD in primary care. The statements have been listed in a Table in a Q&A format, which is a useful quick glance for clinicians. Here is the full text https://www.tandfonline.com/doi/full/10.1080/1750743X.2025.2548754#abstract
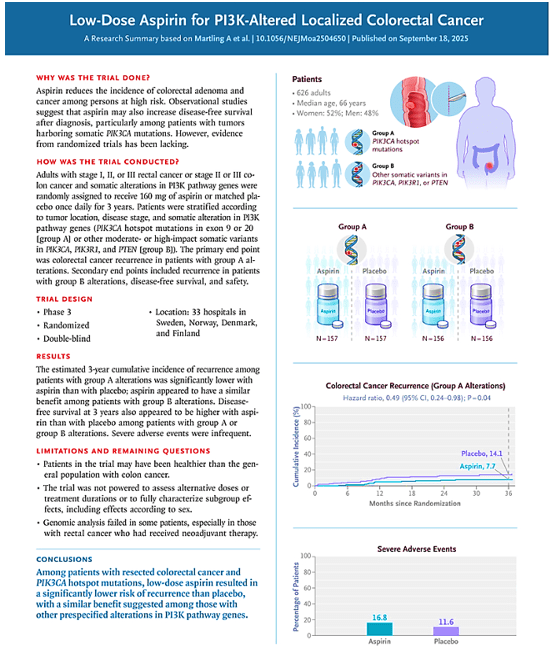
20 Sept 2025: Low-Dose Aspirin for PI3K-Altered Localized Colorectal Cancer
In this study, aspirin led to a significantly lower incidence of colorectal cancer recurrence than placebo among patients with PIK3CA hotspot mutations in exon 9 or 20 and appeared to have a similar benefit among those with other somatic alterations in PI3K pathway genes. Link to the full text https://www.nejm.org/doi/full/10.1056/NEJMoa2504650
17 Sept 2025: In patients with HFrEF and COPD, beta-blocker (metoprolol, bisoprolol, carvedilol, or nebivolol) use is associated with lower risk of cardiovascular death/total heart failure hospitalizations
This real-world study, with a large sample size of 5084 patients with HFrEF and COPD, proves that in patients with comorbid HFrEF and COPD, the significant cardiovascular benefits of beta-blockers outweigh potential concerns for respiratory safety regardless of COPD GOLD group.
Here is the link to the full text https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.70046

14 Sept 2025: 2025 ESC/EACTS Guidelines for the management of valvular heart disease
This update has made some important changes in recommendations for TAVI. Most importantly, the age cutoff for TAVI vs SAVR has been lowered from 75 to 70 years, making it more closer to the American recommendations. Link https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehaf194/8234488?login=false

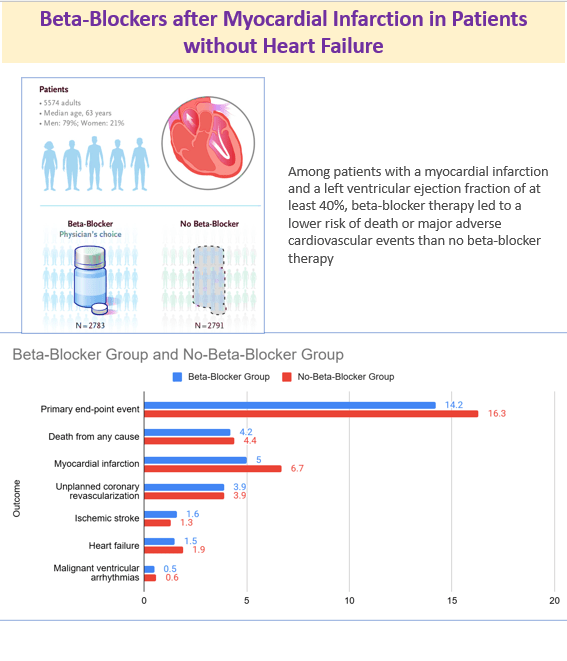
11 Sept 2025: Beta-Blockers after Myocardial Infarction in Patients without Heart Failure
The study showed that among patients with a myocardial infarction and a left ventricular ejection fraction of at least 40%, beta-blocker therapy led to a lower risk of death or major adverse cardiovascular events than no beta-blocker therapy. Link https://www.nejm.org/doi/full/10.1056/NEJMoa2505985
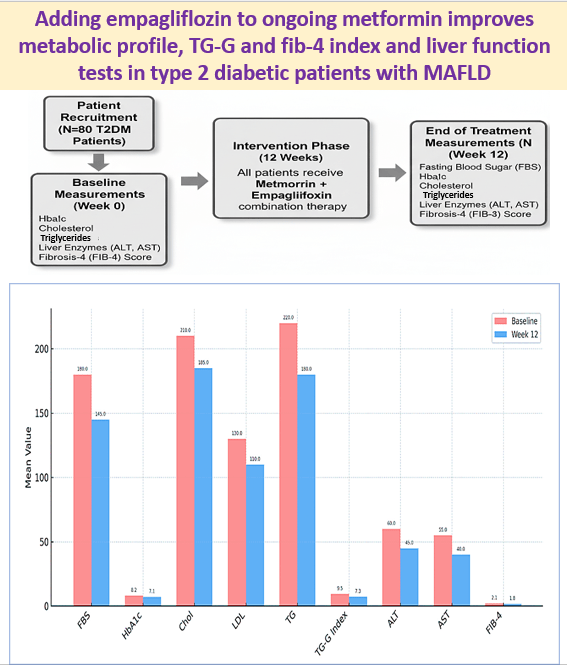
8 Sept 2025: Adding empagliflozin to ongoing metformin improves metabolic profile, TG-G and fib-4 index and liver function tests in type 2 diabetic patients with MAFLD
Adding empagliflozin to ongoing metformin improves metabolic profile, TG-G and fib-4 index: Adding empagliflozin to ongoing metformin significantly improved metabolic and liver-related markers in T2DM patients with MAFLD. Link https://www.tandfonline.com/doi/full/10.1080/17446651.2025.2550733?src=
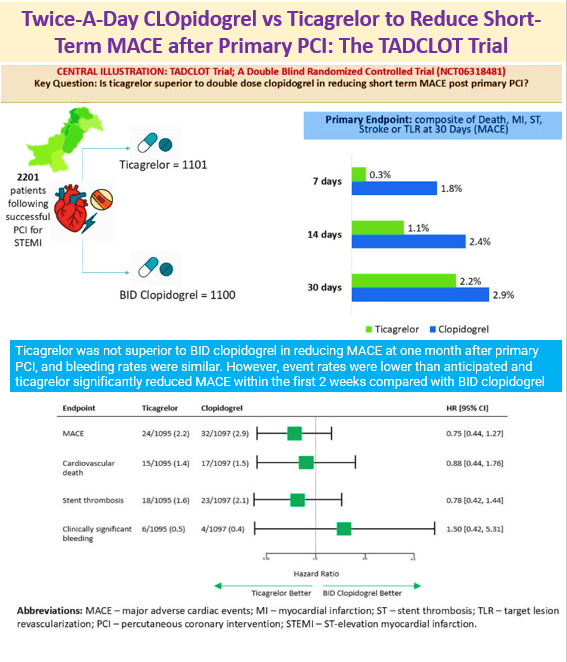
5 Sept 2025: Twice-A-Day CLOpidogrel vs Ticagrelor to Reduce Short-Term MACE after Primary PCI: The TADCLOT Trial
Ticagrelor was not superior to BID clopidogrel in reducing MACE at one month after primary PCI, and bleeding rates were similar. However, event rates were lower than anticipated and ticagrelor significantly reduced MACE within the first 2 weeks compared with BID clopidogrel. Link to the article https://www.jacc.org/doi/10.1016/j.jacc.2025.08.041
2 Sept 2025: 2025 Focused Update of the 2019 ESC/EAS Guidelines for the management of dyslipidemias
An important update is the new risk calculation scores and other parameters of risk estimation. Another important one is early. intensive intervention in ACS rather than step-wise approach. Full text link https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehaf190/8234482?login=false
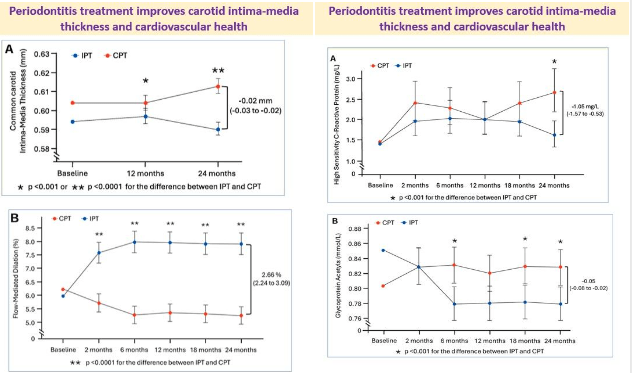
31 Aug 2025: Periodontitis treatment improves carotid intima-media thickness and cardiovascular health
Did you know that treatment of gum disease can improve cardiovascular health?
This is exactly what a new study has shown
Patients: 135 patients with periodontitis
Treatment: Intensive periodontal treatment (IPT) including scaling, root planning, and, when appropriate, surgical corrective therapy or control periodontal treatment (CPT) including supra-gingival scaling and polishing
Carotid intima-media thickness (cIMT), vascular phenotype, and inflammatory markers evaluated over 2 years
Treatment of periodontitis improved endothelial function, reduced systemic inflammation and oxidative stress, and favorably modified structural vascular health
The article also explains why and how the improvement occurs. Here is the full text https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehaf555/8237946?login=false