In diabetes, DPP4-inhibitor is often the first class that comes to mind when metformin and sulfonylurea have failed to control HbA1c or when they are not tolerated.
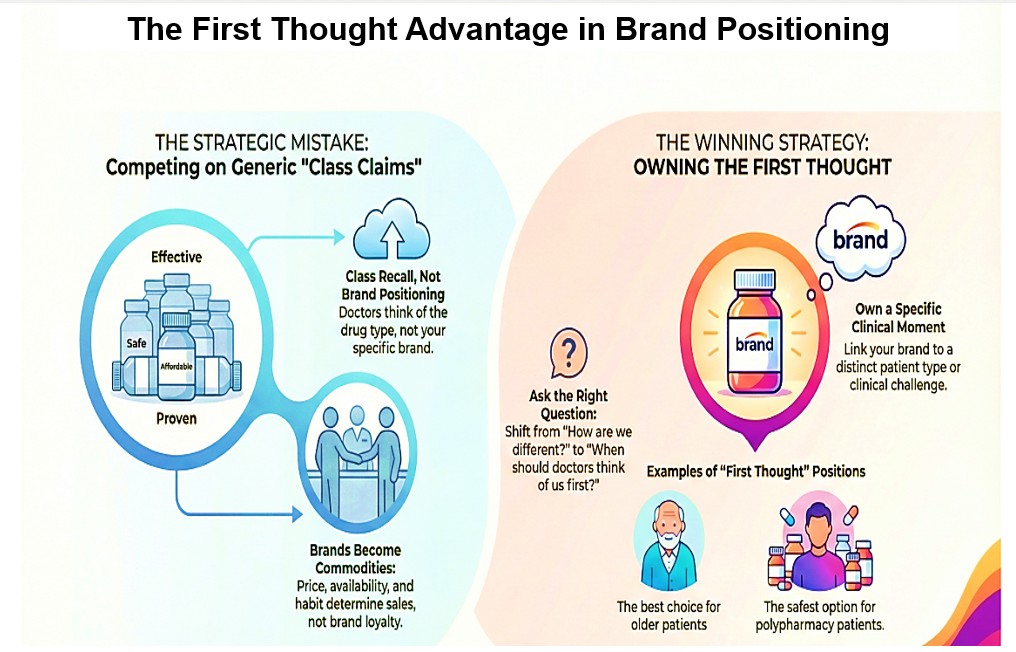
But here is the uncomfortable truth: Class recall is not brand positioning.
Almost all DPP4-i brands say some version of:
- “Effective HbA1c reduction”
- “Affordable”
- “Proven molecule”
- “low risk of hypoglycemia”
- “better than sulfonylureas”
- “Trusted for years”
- “guideline recommended”
These claims describe the class, not the brand
The Strategic Mistake Most Teams Make
They ask: “How do we differentiate our DPP4-i from other DPP4-is?”
The better question is: “At which exact moment in the doctor’s thinking should only our brand surface?”
That moment is the first thought.
Hence, “Owning the First Thought” matters for a DPP4-i brand. A brand should own the specific clinical moment that triggers recall. Some examples:
- The DPP4-i I don’t hesitate to use in older patients
- The DPP4-i I am least worried about (The First Thought When Hypoglycemia Anxiety Is High)
- The DPP4-i that still works when others have ‘failed’ (The First Thought in Long-Standing Diabetes)
- The DPP4-i that can be safely given to patients on polypharmacy
- The DDP4-i that can be given to fragile patients without fear of weight loss (The first thought in sarcopenic patients, patients with history of falls)
Ask a physician: “In this type of patient, which DPP4-i comes to mind first?”
If the answer is:
- “Any of them” → it indicates no brand positioning
- A specific name → first-thought ownership exists
If your brand only appears after comparison, you are already a commodity. Availability, price, and habit will decide your fate.
Strong brands don’t wait to be chosen. They answer one silent question early

